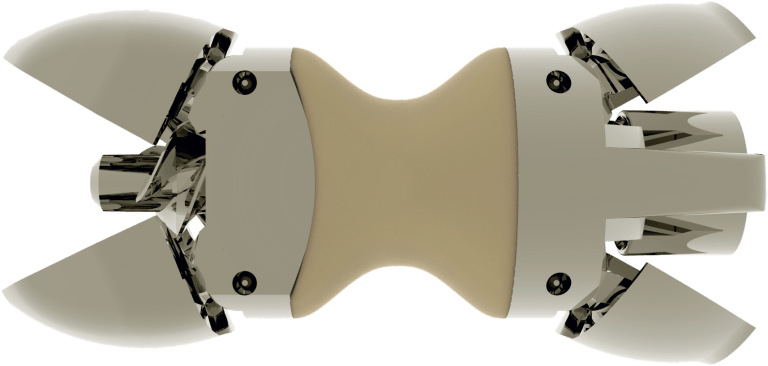
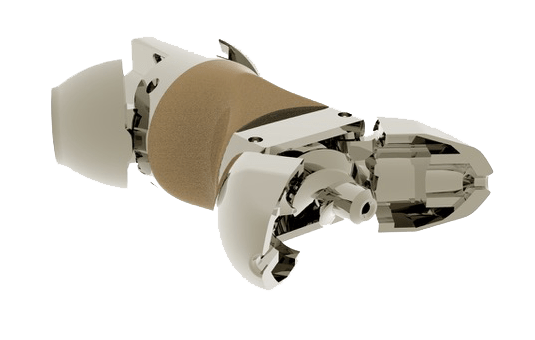
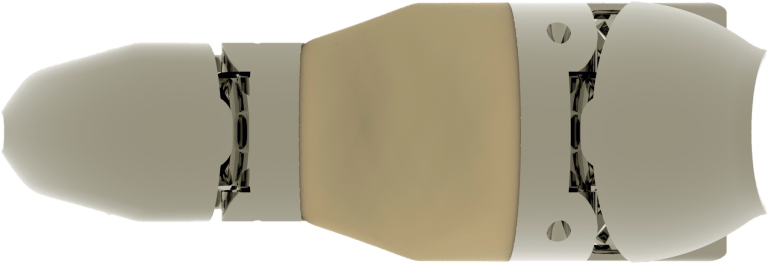
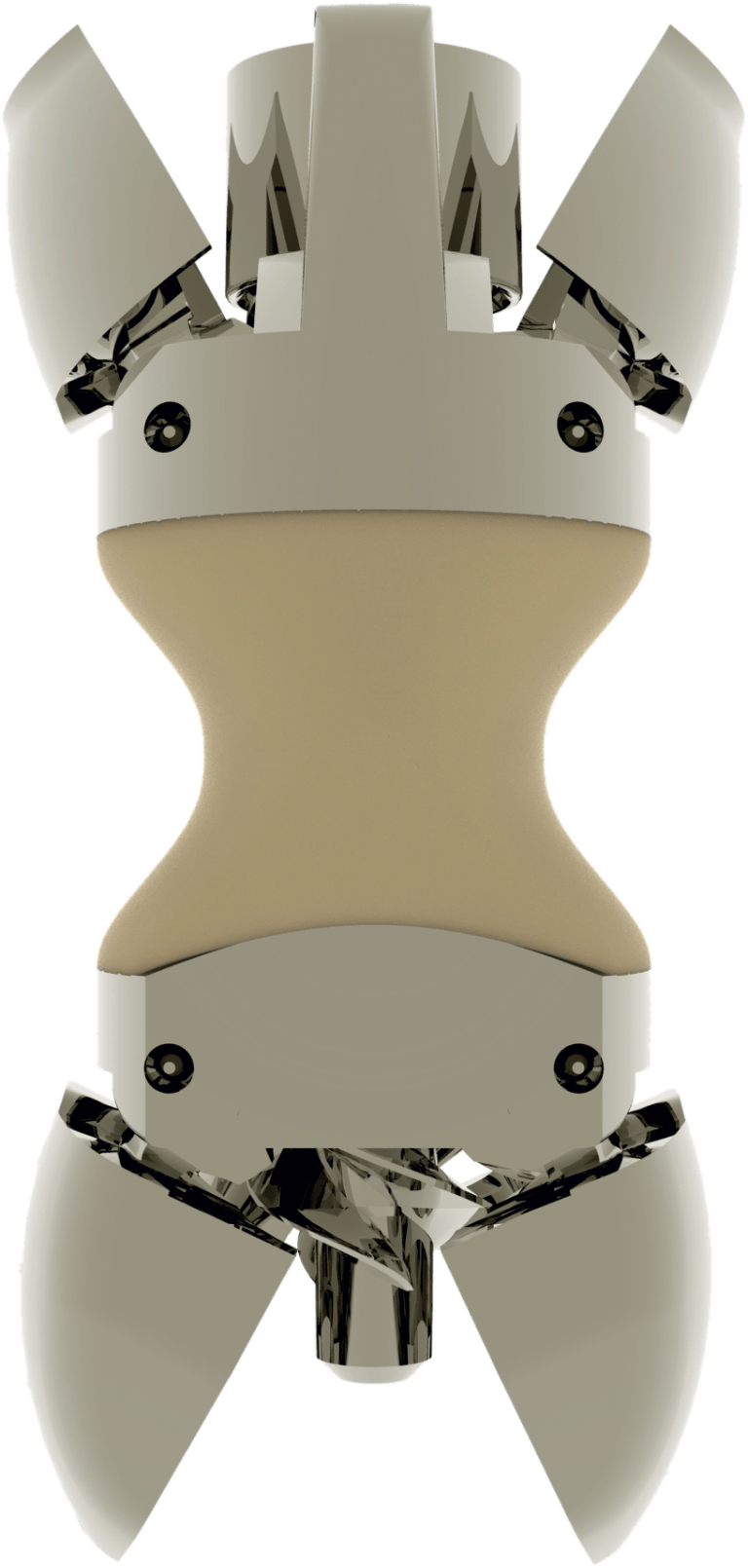
The distance existing between the conservative techniques and the “open” surgery finalized to spinal fusion has been filled with Lobster®, the first dynamic percutaneous interspinous spacer, optionally removable after being implanted. The device is indicated in the treatment of degenerative lumbar canal stenosis, which causes dull ache or acute back pain, which may radiate to the lower limbs with weakness in the legs and loss of balance during walking (claudication neurological).
Through mini-invasive percutaneous technique, the Lobster® device allows the indirect decompression of the spinal canal; it determines the reduction of the freedom of movement in extension of the treated vertebral bodies while keeping the normal rotation capacity and spinal flexion axis. This allows the distension of the posterior portion of the column reducing the eventual disc protrusion and the thickness of the yellow ligaments. These effects increase the size of the spinal canal with reduction or resolution of the associated pain.